Our BSA Audiometry course is a great place to start when you wish to learn how to do a basic audiogram. For those of you that are training to be an audiologist then we offer a masking course too. Please look at our training calendar for dates for these Training Calendar – TJ Audiology Training. We will soon be offering masking theory as an online tutorial, through a portal accessed from our webpage (watch this space)
So, you understand how to do an audiogram but what do the results mean? What are they telling me? When I started audiology 30 years ago, we had a great text book by James Jerger called Clinical Audiology (easier to read than Katz!!) that gave you both audiograms and tympanograms for different types of hearing loss and this helped give you a starting point. Its long out of print now. However, we still regularly use his classifications for our tympanograms.
I am not going to explain an audiogram graph and the different symbols (AC: Air Conduction and BC: Bone Conduction) and degrees of loss, I am assuming that you already have this knowledge! Let’s, start simple and then get more complex (because there is so much information to give this will be an ongoing series). Remember the list is not exhaustive and you will get people that don’t fit the normal pattern. This is why the BAA Onward referral guidance – British Academy of Audiology |British Academy of Audiology has red flags for referral onto ENT, include other audiological issues such as dizziness, tinnitus and facial palsy, not just the audiogram.
Normal Hearing
Please note if hearing is normal but there are other red flags such as dizziness or unilateral or pulsatile tinnitus onwards referral will be required (if these red flags are present for any of the hearing loss below then onwards referral to ENT will still be needed). You would generally expect normal tympanometry results.
Sensorineural Hearing Loss
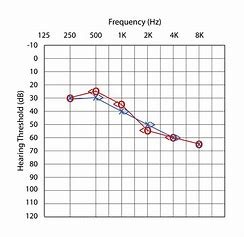
Sensorineural. The triangles which are the bone conduction results are within 10dB of the air conduction thresholds indicating that this is a mild to moderate sensorineural hearing loss. You would generally expect normal tymps with this loss.
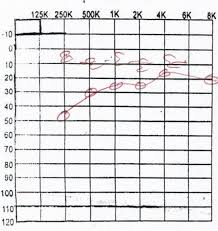
Noise Induced Hearing Loss
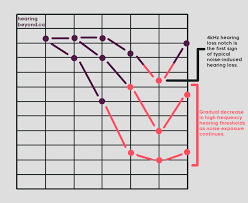
With a noise induced loss you will see a dip between 3-6kHz and then upwards improvement and the BC results within 10dB of the AC (only AC shown on these examples). However, as a client ages, then you add an age-related loss on top or increasing noise exposure (as shown in the 2nd graph) then the proportions will change. You would generally expect normal tymps.
Glue Ear


Glue ear is often found in children under the age of 7-9. The eustachian tube is narrower and flatter than in an adult. Children under this age are more likely to suffer from Glue ear/Otitis Media as the eustachian tube is unable to drain as effectively.
The audiogram with show reduced hearing through the headphones (AC), but the bone conduction results (BC) will be within the normal range. (20db or less if there is no underlying sensorineural hearing loss). You will either have a flat tymp or negative middle ear pressure for the reasons explained below.
The audiogram gives a flatter presentation when the middle ear is so fluid filled that both mass (how much mass is there in an object) and stiffness (how stiff the object is) are being affected. Stiffness affects the lower frequencies and mass the higher frequencies. If there was some draining or improvement in the glue ear than you would see the higher frequencies improve. (as there is now less mass). (31) Acute Otitis Media – FRCS ENT Exam Essentials – YouTube explains otitis media. For information sheets please see Glue Ear – Otitis Media with Effusion (OME) | ENT UK
Tympanosclerosis

Tympanosclerosis is scaring on the eardrum. The scarring occurs either from perforations that have healed or from having had grommets. The amount of scarring will be dependent on the amount of irritation and bleeding that has occurred during these events. Scarring will cause the eardrum’s movement to be stiffer. Stiffness as we said earlier will affect the lower frequencies as shown in the audiogram. Tymps may show restricted or shallow movement.
Perforation
Remember this is an example audiogram and your audiograms may differ . In this case the client already has an underlying sensorineural hearing loss (the BC is out of the normal range). The degree of conductive component of the loss will be dependent on how the perforation affects the transmission of sound from the middle ear space to the cochlea. As for tympanometry you will have either a flat tymp with a large canal volume or you will not be able to obtain a seal. Below is another audiogram example for a perforation where the squiggly lines (masked BC are within normal and the AC is down).