What a strange title to give to part 2 of this series! I have used this title as they are the audiograms that I talk about often, that people either miss or mistake for something else. In all cases except for some of the malingers it led to unnecessary emotional stress for the client’s involved.
Collapsed Ear Canals
Tracy who started TJ Audiology Training and no doubt many others, say that I harp on about this incessantly, and I am happy to admit I do! I think it is a real issue that we miss far too often. One research study on over 300 individuals aged between 3-97 years found that ear canal collapse was observed in 11.4% of their subjects. Prevalence ranged from 6.3% to 36.6%. With the higher percentage score being for the over 75’s. More males than females they found had the problem.
So why is this such an issue for audiograms? Canal collapse will mimic a conductive or a mixed loss. This can then lead to unnecessary ENT appointments and investigations, when all along it was a collapsed canal. This makes us as audiologists look bad if we haven’t seen it. It’s is in some cases an unnecessary referral/cost for MRI’s and ENT time. Even more importantly the personal stress to the client, who is now being investigated for a potential ear pathology cannot be underestimated.
Let’s, talk about how to check for it. Firstly, when we do otoscopy, and you are looking behind the pinna, look also at the opening to the ear canal. Is it narrow? If it is press on the middle part of the pinna. If the canal narrows, you potentially have a collapsed canal.
Client history may also be a dead giveaway! Clients, with collapsed canal will often complain that ear buds don’t stay in or are uncomfortable or they have to use the smallest ear bud. Some will even notice if they press the phone to their ear, they hear worse.
What happens during an audiogram with a collapsed ear canal?
- The pressure from the earphone can partially or fully close the ear canal
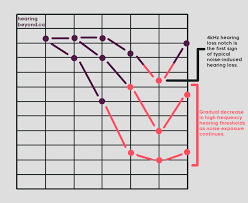
- This can cause increased hearing thresholds, especially at high frequencies
- The results can mimic other conditions, like noise-induced hearing loss
- Client hears you better than their audiogram would suggest.
- If the client already has hearing aids, they will often complain the hearing aids are too loud and/or occluding, and come back for numerous adjustments and the settings of the aids will end up being under target.
- They will often have normal tymps despite the conductive loss.
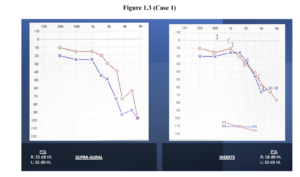
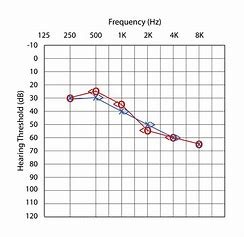
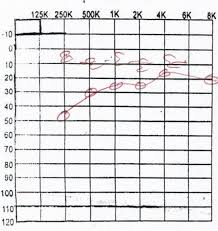
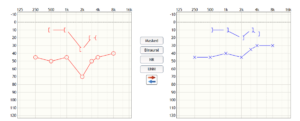
Example 1

Example 2
Above are 2 example audiograms. You can see how in case 1 the higher frequencies have been affected (from Collapsed Ear Canal and Sudden Sensorineural Hearing loss) In case 2 which was a severe canal collapse, it has affected all frequencies. Case 2 is exactly one of those cases where multiple investigations occurred before they realised the issue. (from Bilateral Conductive Hearing Loss due to Collapsed Ear Canals in a 35 Years Old Female – MedCrave online).
As we have said previously mass (a canal collapsing over itself) will affect the higher frequencies which is why we see in case 1, the higher frequencies are down. If masked bone had been done on the supra-aural audiogram there would have been an air bone gap. The audiologist in this case realised it was a collapsed canal and then used inserts hence why there is no masking or BC.
In case 2 it’s a complete collapse causing both stiffness and mass and hence why there is an airbone gap across all frequencies. However, it is worse in the higher frequencies this is another clue!
In both cases tympanometry results were showing normal middle ear movement.
What to do if you don’t have inserts?
Not everywhere has inserts. Some people have used speculum to hold the canal open and then put headphones on top. This can be uncomfortable. I have found using tympanometry tips work best (as big as is comfortable). Cut off the flange part of the tymp tip, tie cotton string through it and knot it; and then insert. The cotton string makes taking it out so much easier. Always note on your audiograms that you have found collapsed canals. This ensures that all individuals attending to this client now and in the future are aware of the issue.
Let’s fool you audiogram
This audiogram occurred when I was working in the NHS. Whilst it is possible that the loss occurred post operatively. I find that unlikely as the previous audiograms hinted the underlying loss.
As it was a child people suspected it was due to slight inattention/boredom during a hearing test (the child was under 7). As you can see pre-operation both sides have a conductive loss. However, the right side is showing a mixed loss at 2000Hz. Staff though this was a false positive. Look at the audiogram below though, there is a hint that this may be sensorineural, even if the BC is incorrect. Why is the AC dip so much worse than the adjacent frequencies at 2000hz on the right? Tymps were flat in this case.
Pre-operative
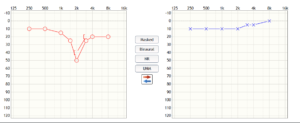
Post operative
I strongly suspected that I would get the above audiogram as the 2 previous audiograms had shown the dip in AC & BC at 2000Hz to varying degrees. The dip at 2000Hz is out of proportion to the other frequencies around it, yes it can be fake if it isn’t repeatable to some degree. Given that the dip, stayed in all prior audiograms should have alerted to all that there was potentially an underlying sensorineural hearing loss at 2000Hz on the right. The child reported much better hearing post operatively but still some issues in noise. Needless to say, it was a shock to both the mother and the child. This result did not change post grommets falling out or in later tests. Unfortunately, I wasn’t able to find out the probable cause of the sensorineural dip at this frequency.
I always say if it doesn’t look right, it isn’t right. This dip at 2000Hz was consistent. It is rare for people to fake the similar levels of an audiogram well over a series of hearing tests.
The malinger!
Malingering means not giving a true result. There are many different reasons for this. It could be due to attention seeking, psychological issues, misunderstanding instructions, or wanting compensation for their hearing loss. Jerger, in 1981 came up with the below statistics, in brackets are my suggested reasons.
- 2% of population
- 7% in children age 6-17 years
- Typical mean onset of NOHL = 10-12 years (school stress, sibling has hearing loss)
- Rare below 7 years of age (as children under this age seek approval)
- Up to 50% of those seeking compensation
So, what type of audiograms would you see?
Observation
- PTA response pattern
- Audiometric pattern – e.g. flat SNHL or worse than subjective hearing level
- Between ear unmasked level difference greater than 70 dB for AC and 10-20 dB for BC
- History – a lot can be gained by listening to the patient e.g. sibling with hearing loss, exams coming up, trauma.
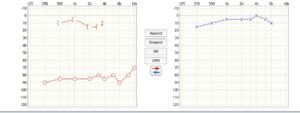
The above audiogram’s AC thresholds on the right were not yet masked. Therefore, this a malingering audiogram. This is because it isn’t possible for there to be more than a 70dB difference between ears without the good ear (left) helping the bad ear. Therefore, we would expect better AC results on the right pre masking than what we are given above. True hearing test results on the right would be better around 60-70dB and deteriorate when rule 1 of masking is applied (more than 40db difference between AC thresholds). Also why is the BC so good particularly if there is no history that suggests conductive loss.
This is an easy one to spot. However, taking a verbal history with a client tells a lot. For example, if you a getting a moderate to severe sensorineural hearing loss but they can still hear you speak with no hearing aids when you turn away, well that isn’t possible!
Also flatter audiograms are easier to fake than a sloping loss. So we see these more with malingering audiograms.
Remember the above audiograms are examples, variations to these will occur given clients otological history. But hopefully I have given you a good place to start.
Next: Part 3 – Middle ear pathologies such as otosclerosis