The key to good fitting custom earmoulds and hearing protection, ITE and CIC hearing aids are accurate ear impressions. Its important to know when you’ve inserted your otostop deep enough down the canal, and that the otostop is pointed in the direction of the eardrum. A good, deep impression means getting to the 2nd bend of the ear canal. Some tell-tale signs that you’ve reached the 2nd bend include a characteristic slip of the otostop into position which often coincides with slight resistance as it enters the bony portion of the canal. When you look on otoscopy, you will see that the otostop is framed by the cartilaginous portion of the canal.
You may wish to mark your otolight. For standard adult ear impressions, mark your otolight placement tool at 16 mm from the tip to guide the otoblock exactly 4 mm past the ear canal’s second bend. For babies under six months old, use a 10 mm marker. I tend to use nail polish so that it stays on the light source. Also remember otolights can get hot. So always turn them off when you are not inserting the otoblock.
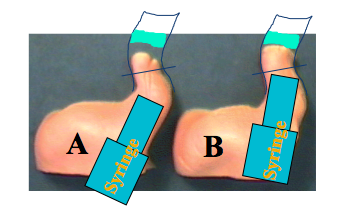
Also, what way are you facing the syringe when inserting. In example A shown below from Audiology Online https://www.audiologyonline.com/articles/making-good-ear-impression-setting-15855 there wont be enough energy for the material to get to the otostop as it using its energy against the canal wall. We want to syringe with minimal pressure so as not to go past the otostop so the placement of the syringe in the canal is critical.
All ear canals are very different from one another and taking good impressions takes practice in fact from the same Audiology Online article is a very good comment below from Michele Hurley, the writer of the article.
“Sometimes there are challenging ears. Every ear, just like snowflakes, is different. We may see some canals that are very curvy; some are very straight. Those all impact how we need to shoot the impression. When you see a very curved ear canal, keep in mind that sound direction is going to be very important in the end product. We need to not only shoot for giving our manufacturer the depth and the angles of those curves, but we also need to keep in mind that sometimes we will need to do some modifications for good retention, as well as comfort with those sharp curves….” This is so important, earmould manufacturers don’t have crystal ball, so letting them know directions or any lumps and bumps that need to be shaved down for a good fit means less remakes for them, you and the client.
Patient/client safety is paramount and the British Society of Audiology has a recommended procedure for impression-taking in adults/children over 5 years of age and for children under 5 years of age. https://www.thebsa.org.uk/guidance-and-resources/current-guidance/
Louise Hart holds 1-day BSA accredited impression-taking courses at West Berkshire Museum once every 6 weeks for adults/over 5 years and on request for children/under 5 years. Learn how to take impressions safety and accurately according to the recommended procedure, using the correct brace positions during the procedure. Learn about what to look for on otoscopy and experience how to know when you’ve reached the 2nd bend.
Find out about Louise Hart and take a look at the website: www.tjaudiology.com
This is a brilliant article below from Neupsy Key Admin on how to write your clinical notes. Neupsy Key is a search engine for neurology, neurosurgery, psychiatry and psychology. I use their website quite often in my research on topics https://neupsykey.com
Before you read their article below remember: If you haven’t documented it, it didn’t happen. Your clinical notes are important guide to what has occured in the appointment; and can be used in a court of law if required. If you haven’t written it down, the law will say there is no documented evidence that it occured. So for your sake and your client it is important that your notes are an accurate indication of what occurred and what was discussed in the appointment.
Learning the Rules of Documentation: What To Include, What To Skip
Medical documentation is where clinical reasoning becomes visible. It’s how teams coordinate care, how risk is managed, and how decisions are justified when questions arise later. Done well, documentation improves outcomes and reduces errors. Done poorly, it can confuse the next clinician, weaken continuity of care, and create unnecessary legal exposure.
The challenge is that many clinicians were taught how to write notes, but not how to edit them. Notes often balloon into copy-pasted templates, duplicated histories, and exhaustive just in case text that hides the real story. The goal is not more documentation. The goal is the right documentation: accurate, relevant, timely, and readable.
You may also encounter non-clinical pressures, from time constraints to billing requirements to administrative expectations. Some learners look to writing resources such as https://writepaper.com/ to structure complex text. Still, medical notes have their own rules: they must reflect real clinical work, respect patient privacy, and support clinical decision-making without turning into a novel.
Below are practical rules for what to include, what to skip, and how to make your documentation clinically useful and defensible.
Document for Patient Care First
A medical note is primarily a communication tool. Your future self and your colleagues should be able to answer three questions quickly: What is happening? What did we decide? What are we doing next?
Start with the patient’s current problem, not the entire history of medicine. A well-structured HPI, assessment, and plan should make the clinical arc obvious, including relevant positives and negatives. If you are writing a consultation or inpatient note, clarify the question you are answering and the decisions you are making. If you are writing outpatient notes, tie symptoms and function to the plan and follow-up.
When care is shared across disciplines, focus on the information that others need to act safely. For example: medication changes, safety concerns, pending studies, red-flag symptoms discussed, return precautions, and follow-up timelines.
Include Decision-Making, Not Just Data
Data without interpretation is noise. Anyone can list labs; fewer can explain why they matter. Good documentation captures clinical judgment, especially in high-risk scenarios and when the plan is not obvious.
In the assessment, show your differential diagnosis when appropriate, the reasoning behind your working diagnosis, and the rationale for key decisions. If you choose not to pursue a test or treatment, document why (for example, low pretest probability, potential harms, patient preference, guideline-based reasoning, or prior results). This is especially important in neurology and psychiatry, where symptoms can be complex, overlapping, and longitudinal.
Also, document uncertainty appropriately. Rule out language can be misused; instead, state what you considered and what you will do if the situation changes. Think of your note as a record of how you managed risk.
Be Specific About Time, Severity, and Function
Vague notes create problems: “doing better,” “stable,” “denies symptoms.” Better documentation includes objective anchors. Time course, severity, triggers, and functional impact should be explicit. In neuropsychiatric contexts, function is often the most meaningful outcome: sleep, work, school, cognition, independence, safety, and social engagement.
Be careful with blanket statements if the encounter did not actually cover them, or if they conflict with the HPI. Contradictions are credibility-killers. Instead, document targeted negatives that matter for the differential and red flags that were assessed.
For mental health and cognitive concerns, include concrete examples: frequency of panic episodes, number of hours slept, missed workdays, falls, medication adherence, episodes of confusion, or caregiver observations. Specificity supports both clinical care and medical necessity.
Skip Template Bloat, Copy-Paste, and Irrelevant Detail
Overdocumentation is not safer documentation. Excessive templated text can obscure key findings and introduce errors, especially when copied forward without careful editing. If the note becomes difficult to read, critical details are more likely to be missed.
Skip content that does not change management or clarify the clinical picture. Avoid duplicating entire prior histories unless you are updating them. If you must copy forward for continuity, summarize and confirm what is still true, and update what has changed.
Also, avoid documenting sensitive information that is not clinically necessary. In neuropsychiatric settings, this includes unnecessary third-party allegations, stigmatizing language, or speculative diagnoses. Document facts, patient-reported statements, observed behavior, and clinically relevant context, while maintaining respect and neutrality.
A helpful internal filter is: If another clinician read this sentence, would it help them treat the patient safely, justify the care provided, or understand the patient’s trajectory? If not, consider deleting it.
Consent, Capacity, and Patient Communication Notes
Some of the most important documentation is about what was discussed, not what was ordered. Notes should reflect informed consent and shared decision-making when relevant. That includes risks, benefits, alternatives, and the patient’s questions and preferences, especially for invasive procedures, high-risk medications, and discharge decisions.
Capacity assessments and safety planning should be documented clearly and objectively. If a patient declines a recommendation, document what you recommended, the patient’s stated reasons, and your counseling on potential consequences. Avoid judgmental language; keep it clinical.
Include key communication elements that reduce misunderstandings later: return precautions, follow-up plan, and what symptoms should prompt urgent evaluation. If family members or caregivers are involved, document who provided the history, what they observed, and what was communicated to them, within privacy boundaries.
Practical Checklist for Clean, High-Value Notes
When you’re pressed for time, it helps to have a reliable checklist that keeps notes concise without missing essentials:
Identify the primary problem and the clinical question
Include relevant history, exam, and key data tied to that problem
Document your assessment with reasoning and risk considerations
Write an actionable plan with responsibilities and timelines
Record consent, counseling, and patient preferences when relevant
Remove duplicate, templated, or irrelevant text before signing
This approach supports care quality and also aligns with documentation expectations used in audits, peer review, and medico-legal settings.
Conclusion: Write Notes That Tell the Truth and Tell the Story
The best medical documentation is factual, focused, and defensible. It prioritizes patient care communication, captures decision-making, and preserves the clinical narrative without burying it in clutter. If you want a simple rule: document what you did, why you did it, and what happens next.
As you refine your documentation habits, aim for notes that a colleague can read quickly and trust completely. That means fewer copied blocks, more intentional summaries, and clearer rationale. Over time, your notes become not just records, but tools: they improve continuity, protect patients, and reflect the quality of your clinical thinking.
Louise Hart joins Tracy James to deliver tinnitus and hyperacusis services to adults and children from October 2020. She will also be providing her expertise in our training courses delivered to provide British Society of Audiology Certificates in impression-taking, hearing surveillance and audiometry and tympanometry.
Louise says ‘ I am excited to be providing more independent work, alongside my NHS work. I really enjoy training and have pride in helping individuals enable their skills to the recognised standard of the British Society of Audiology. We will be training GPs, teachers of the deaf, assistant audiologists and any professional who works in the hearing industry, and I look forward to meeting our new delegates at the next course in Newbury.’
‘With regards to tinnitus, I will be providing the only independent tinnitus and hyperacusis management service in West Berkshire at Tracy James Hearing. We know the earlier we intervene in helping people manage their tinnitus and hyperacusis the more successful the outcome for them’
Despite research on drug or physical interventions on tinnitus, at present none seem to consistently reduce tinnitus well enough; this is why management techniques are used to combat tinnitus. For over 20 years chronic pain sufferers have successfully been using cognitive behavioural techniques to manage pain, and we now have more studies showing the same success with tinnitus.
Louise will tailor a programme to you to help your tinnitus and/or hyperacusis; these can be provided face to face or through video consultation. For further information on tinnitus and or to book an appointment, go to Tracy’s website tjhearing.co.uk.
For further information on audiology training courses, go to tjaudiology.com
Otis the virtual patient (from Innoforce.com) can be used to practise basic audiometry and tympanometry and masking. We use it in our classes and its a great way of developing your skills in audiometry without having the pressure of time or the client’s ability to focus, while getting used to the controls and techniques required. If you’re learning how to carry out masking, it is an invaluable learning and evaluation tool and you don’t need to rely on your supervisor to explain results.
Otis is a little bit like a real person, for example, your client can fall asleep if you take too long or shout if you present sounds that are too loud. You can view your otoscopy, history and tymp data as part of the assessment. There is reference data for masking and symbols. You have real-time evaluation and assessment of your procedure as you do the audiometry – it tracks your accuracy, time and errors. You can also progress from easier audiograms, to more difficult cases.
In this post I would like to share some thoughts about rule 3.
This is the rule that many people scratch their head over, mainly because it can be difficult to see, but also because it doesn’t come up that often (and generally only in more complex cases). Therefore, if you’re used to testing routine cases you may not have to think about rule 3 very much. That’s why it’s good to refresh your knowledge so that you don’t miss it when it does come along. Completing rule 3 means that your hearing test will be more accurate; the end result may affect your diagnosis and also your hearing aid prescription.
How does Rule 1 differ to Rule 3 in masking?
We know that Rule 3 is only needed when Rule 1 has not been carried out and that both involve air conduction masking. But why?
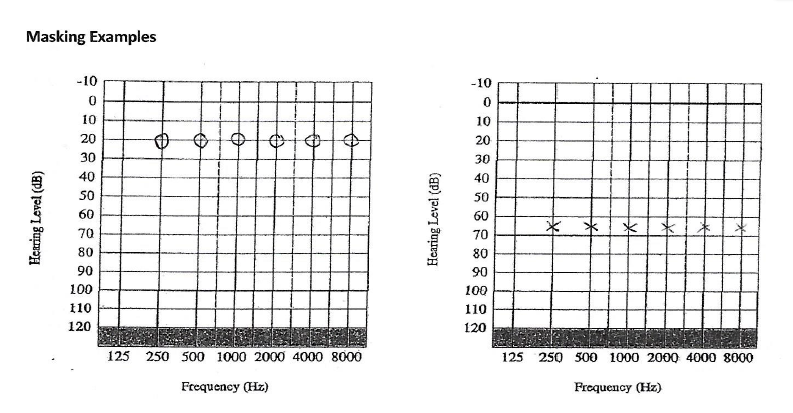
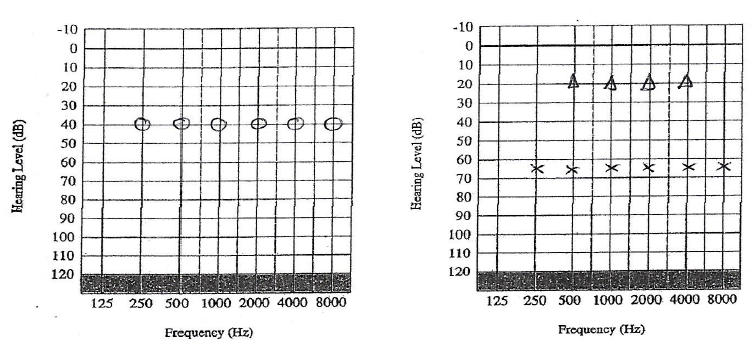
Masking is carried out when there is a difference of 40dB between cochleae when using headphones. When we look at Rule 1 the difference between the two cochleae are obvious:
We mask the air conduction, and find the following:
Rule 1 was carried out at all the frequencies as there was a difference of >40 dB at all the frequencies between the 2 ears. Headphones were used and the left ear was the test ear, and the right ear was the non-test ear, to be masked.
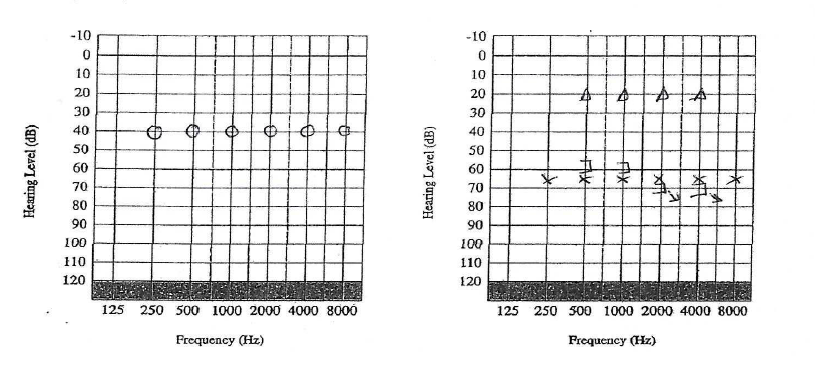
However, the difference between the two cochleae can be hidden when the non-test ear has a conductive component. Say for example the same patient as above comes back a few weeks later with a hideous cold that has affected his right ear.
There was no need to do air conduction masking in this scenario (Rule 1 not required).
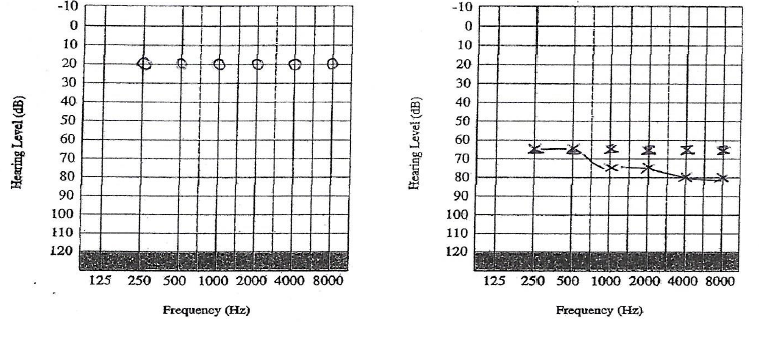
Bone conduction was carried out on the worse ear:
As the there was an air bone gap of >10dB between the air and bone conduction thresholds (Rule 2), bone conduction masking needed to be carried out at 0.5, 1, 2 and 4 kHZ. The left ear was the test ear using bone conduction, and the right ear was the non-test ear, to be masked.
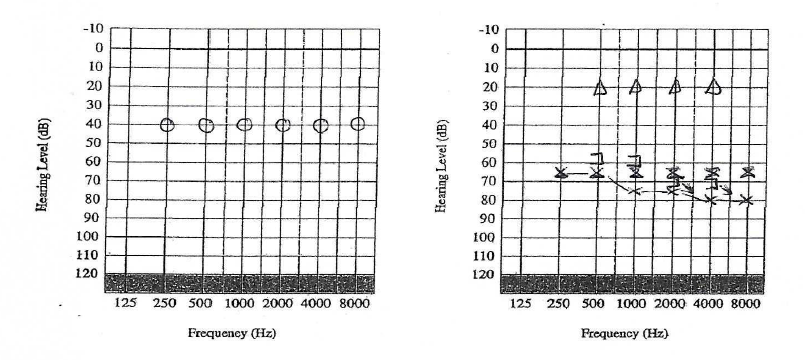
Once bone conduction was completed, we could see an asymmetry once again:
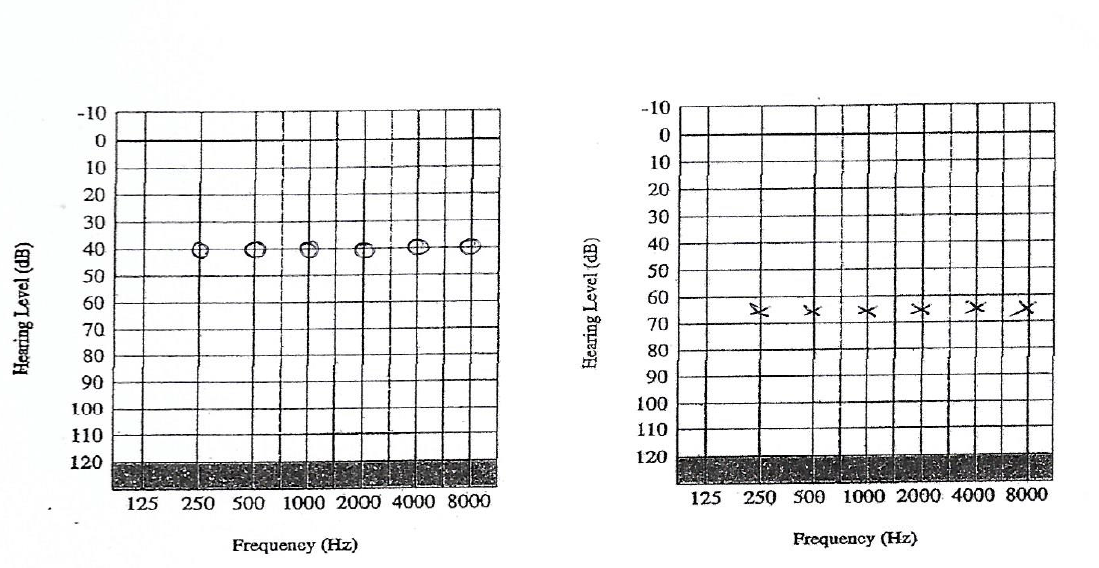
In this case we could only see that the right cochlea was >40dB better than the left cochlea because bone conduction had been completed. So we went back to using headphones again and masked the air conduction, with the masking noise in the right ear (non-test ear), and retested the hearing thresholds on the left ear (test ear). This revealed the following:
Moderate to severe sensorineural hearing loss on the left. Mild conductive hearing loss on the right.
Rule 3 explained? (Some tips):
Rule 3 is usually required because the non-test ear has a conductive component
The asymmetry that is present between the 2 cochleae (as you would visibly see in Rule 1) is hidden until you carry out the bone conduction. That is why you only carry out Rule 3 if Rule 1 has not been carried out.
Rule 3 is often missed because the BC that relates to the better ear (non-test ear) is recorded on the side on which the BC is placed (worse ear). Therefore you have to think to which ear the not-masked BC belongs to.
Although you check the BC to ascertain an asymmetry, you don’t use the BC in your masking procedure – you are masking the AC thresholds only.
At frequencies where no b-c thresholds have been measured – if there is a possibility that a-c threshold at these frequencies (including 250 Hz and 8000 Hz) are not the true thresholds, they should be masked.
If you have any questions please send an email to admin@tjaudiology.com and either Tracy James or Louise Hart will get back to you
Tracy James of TJ Audiology delivered a 3 day BSA certificate training course in Audiometry and Tympanometry at Medivar in Tallin, Estonia. Tallinn was fantastic, with a beautiful old town; cobbled streets, 14th Century buildings and lots of history. Estonians are also very exotic with only 1 million inhabitants. For those of you that don’t know – Estonians speak Estonian which has a lovely sing song lilt to it.
The training course was delivered to 5 employees in English and I was amazed at how those on the course (and Europeans in general) were able to use English in their day to day lives. Everyone took great assurance in having lots of practice time and as the group was small, there was lots of time to make sure that questions could be answered. Some of what we covered included anatomy and physiology, otoscopy images (possible abnormalities we may come across), contraindications, physics of sound as well as the practical procedure.
Feedback included: “Very thorough and in-depth. Informative, professional and gave consistent support and feedback to the practical assessments as well as to how we were progressing in general. Pace was perfect.”
I was pleased to have visited both Estonia and Medivar and to learn more about Estonian culture as well as Audiology Services. Medivar is a European distributor of health equipment, including Audiology equipment and supplies. I found the people I worked with there very professional and I was very well looked after. Thank you very much!
The HSE indicates there is variation in practice and standard across practitioners in Hearing Surveillance Programmes. Does your occupational health worker attend a British Society of Audiology accredited course?
Tracy James MSc
The Health and Safety Executive (2013) carried out visits and questionnaires across a range of health surveillance programmes across the UK so that current practices across teams and individuals could be evaluated. Their key findings included that there was variation in practice across practitioners and health surveillance programmes. In particular, they noted that:
‘….some practitioners probably did not adopt sufficient measures to exclude the effects of prior exposure to noise and background noise when the test was being conducted’
…and with regards to training competency they noted:
‘If practitioners had undergone appropriate training there is an assumption that they would be competent to undertake otoscopy, but it was found that otoscopy was not always carried out before testing’
HSE (2013). Current Practice in Health Surveillance for Noise, pp iii
The Health and Safety Executive (HSE) outlines clearly what is required with regards to a health and surveillance programme under the Guidance on Regulations ‘Controlling Noise at Work’ 2005. In Appendix 5 it reports that a training syllabus for industrial audiometricians has been prepared by the British Society of Audiology (BSA) which has accredited a number of courses. The document is available https://www.thebsa.org.uk/wp-content/uploads/2023/10/OD104-65-Surveillance-Audiometry.pdf
Why choose a BSA accredited course? In order to be accredited, the provider has submitted the course content and assessment material to experts in the field to ensure that the training is accurate and according the recommended procedures published by the BSA. It also ensures that the minimum training guidelines are fulfilled and that the trainer has a suitable background knowledge/qualifications for providing the training. A representative of the BSA will also visit the course provider during their training programme. In order to remain accredited, course providers are required to resubmit their training material every 3 years to ensure the course is up to date.
BSA industrial audiometry courses are designed to enable occupational health workers to:
Undertake a brief subject interview and/or administer a questionnaire regarding otological and noise history
Perform otoscopy and pure-tone a-c threshold audiometry without masking, both in accordance with BSA recommended procedures. Audiometry may be manual or automated
Interpret results and classify them in accordance with HSE guidelines
Relay information to subjects and, with consent, to the employer or other person with overall responsibility for that particular hearing test program.
Make appropriate 3rd party referrals
BSA (2008)
Has your occupational health worker completed a BSA accredited course in industrial audiometry? When you scroll online you can see many courses that quote their course is ‘BSA approved’ or ‘based on’ BSA guidelines or ‘follows’ BSA recommended procedures – but they’re not actually accredited! The BSA lists the accredited courses available nationally on https://www.thebsa.org.uk/wp-content/uploads/2023/10/OD104-26-V8-Accredited-Course-Providers-July-2022.pdf or you can check your course is accredited by contacting bsa@thebsa.org.uk.
A BSA accredited course may the key to enable consistency in training and competency levels across practitioners within a hearing surveillance programme. Choose your course and make sure it is accredited. The BSA (2008) recommends that the occupational health worker attends a refresher course in industrial audiometry every 3 years.
References
HSE (2013). Current Practice in Health Surveillance in Noise.
HSE (2005). Controlling Noise at Work. Guidance on Regulations
BSA 2008. Guidelines on the Training of Industrial Audiometricians.
Tracy James MSc is a Clinical Scientist and co-director of TJ Audiology Services along with Louise Hart, an Audiology Training Service. The next BSA accredited course in Industrial Audiometry is at PC Werth Headquarters, London
There are many anatomical differences between the ears of adults and children. For example, children’s ear canals tend to be narrower and straighter. This means you need to consider the equipment you use, for example the size and width of your syringe and the size of your otostop. As babies’ ear canals grow rapidly in the first year of life, you may need to change your equipment as the baby gets older, so you will need to use your judgement on otoscopy. The best view on otoscopy can be obtained by pulling the ear back only in children, since their ear contains more cartilage than adults. You may not recognise a second bend in a child’s ear so you have to learn to ‘feel’ when you have entered the bony portion of the canal.
A neonate ear canal is much shorter than an adult’s therefore the BSA recommended procedure (2013) recommends you use a 10mm marker as a guide on the otolight for babies under the age of 6 months. A cotton otostop is also recommended since sponge may be more abrasive at this age (BSA 2013).
Perhaps the biggest difference in taking impressions in children is the interaction you need with the caregiver as well as the child. There are a range of brace positions that you can try and are documented in the BSA recommended procedure (2013) to ensure that children of different age groups are safe when carrying out the procedure. You also need to make it fun – lots of toys and distractions to keep those little hands busy while the impression material is setting.
So in summary – a range of different sizes of equipment is needed, a good eye on otoscopy to judge the position of the otostop, consider the right brace position, have lots of toys, fun and patience while remaining calm and informing both parent and child as you go along.
It is recommended that anyone carrying out impressions on children under 5 years are competent, and have sufficient training and experience (BSA 2013). Tracy James is holding a 1-day BSA accredited impression-taking course for children under 5 years in Newbury on the 24th of May (Newbury College). Learn how to take impressions in children safely, for different age groups and experience a range of different types of equipment you can use, and learn more about children’s ear moulds.
Find out about Tracy James and take a look at her website: www.tjaudiology.com for more details regarding her courses, or email tjaudiology@outlook.com.
References: British Society of Audiology (2013). Recommended Procedure (Supplement). Taking an impression: children under 5 years of age.
As audiologists we all learn masking as part of our training. But the truth is, the real learning is in the experience of the various hearing losses we come across. Unfortunately for some, we’re not always in the position to reflect with another practitioner about some of the more complex hearing losses – so how can we really learn?
Masking is carried out as a result of the minimal interaural attenuation of 40dB when using headphones, 55dB when using inserts and 0dB when using a bone conductor. As a result, we follow certain rules to decide when masking should be carried out (BSA recommended procedure 2011) to ensure an accurate hearing test is obtained.
We probably know the rules by heart. But…
Why do we need to do Rule 3 and what is it’s relationship to Rule 1? What about central masking and the effect of conductive losses on masking? When are inserts more appropriate than headphones? When do we choose to mask bone conduction on both ears? What is effective masking? Even the most experienced of audiologists have to reflect on such questions when considering best practice.
A training course in masking in audiometry will enable audiologists to consider and understand why we need to mask, rather than just learning the rules. TJ Audiology Services uses audiometry simulation software to practice different scenarios, alongside interpretation of working audiograms. Audiology Courses are available in 2016 at Audiology House, London. Bring yourself up to speed, or start from scratch and benefit from having the time to ask all those questions and more in a safe learning environment and discussion with other colleagues.
BSA Recommended Procedure (2011): Pure-tone air-conduction and bone-conduction threshold audiometry with and without masking.
A hearing test (audiometry) measures the quietest sound and individual can hear, at least 50% of the time – known as hearing threshold level (HTL). An individual’s HTL at different frequencies is recorded in an audiogram for each ear, and this information can be used to categorise hearing as within normal range, or a hearing loss that can range from mild to profound. Otoscopy and tympanometry is used alongside audiometry to identify any abnormalities of the middle ear that may be affecting the hearing, e.g. perforation or glue ear.
In hospitals and hearing aid dispensing practices, audiometry and tympanometry is typically carried out by audiologists who are trained to undertake these procedures during their university course. In the UK, audiometry is carried out according the British Society of Audiology Recommended Procedure.
However, basic hearing tests and tympanometry can also be performed by GPs, occupational health nurses, audiometricians, assistant technical officers, teachers of the deaf and hearing aid assistants. The British Society of Audiology has a Practice Guidance Document for “Hearing assessment in general practice, schools and health clinics: guidelines for professionals who are not qualified audiologists”.
A British Society of Audiology accredited course in basic audiometry and tympanometry trains non-audiologists to undertake hearing tests in the field and interpret the results, according to minimum training criteria.