Acoustic neuroma/ vestibular schwannoma, are benign usually slow maturing growths, that develop on the vestibulocochlear/ eighth cranial nerve. This nerve leads from the brain to the inner ear. It consists of the vestibular and cochlear nerves.
Acoustic neuromas (AN) develop from Schwann cells, these cells are a type of glial cell, which are non-neuronal cells that support the function of neurons, and wrap around and support nerve fibres. They can occur on any cranial or peripheral nerve in the body, but in the brain, acoustic neuromas are the most common.
Acoustic neuromas typically begin growing where the central nervous system transitions into the peripheral nervous system. The incident rate is somewhere between 1-3 % in 100,000 people and may increase in older age.
Many acoustic neuromas don’t grow, and many that do grow tend to develop slowly. Occasionally they can grow quickly, but this is rarer. Unlike cancer tumours they don’t generally invade and destroy tissue. What can occur is that they cause symptoms as they grow and push on surrounding structures. This may be where you see effects on the face and eye. Medscape: Acoustic Neuroma- Practice Essentials
Symptoms
The symptoms of an acoustic neuroma are as follows:
- Unilateral/asymmetrical hearing loss is the most common symptom that leads a client to attend an audiology appointment. Usually progressive
- Tinnitus – Especially if it is unilateral, non-pulsatile
- Vertigo and disequilibrium – Uncommon (may come and go) as the tumour grows it may cause dizziness and then the brain habituates and compensates to the change and the dizziness is less.
- Headaches – Present in 50-60% of patients at the time of diagnosis
- Facial numbness – Occurs in about 25% of patients
- Some acoustic neuromas can present as a sudden (idiopathic) hearing loss (this actually happened to a relative of mine). It’s a less typical presentation but it does occur.
Generally, acoustic neuromas cause ear symptoms on one ear only. For example, the individual may suffer with a sensorineural hearing loss or unilateral tinnitus on one side. Although the tumour usually develops on component of the vestibular nerve, vertigo from it is less common for the reasons I mentioned above. Although the facial nerve is also in the internal auditory meatus, an acoustic neuroma causing facial weakness is not as common as hearing loss or tinnitus. This is because motor nerve fibres around the face are resistant to pressure. Whereas the hearing fibres are thin and more likely to be damaged by pressure.
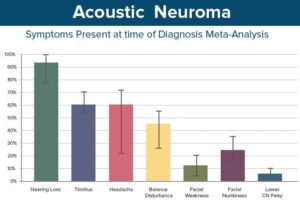
Diagram and symptoms behaviours from : Medscape: Acoustic Neuroma- Practice Essentials
Referral Criteria
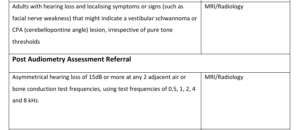
Don’t forget unilateral tinnitus or an unexplained increase in tinnitus in the last 6 months as well.
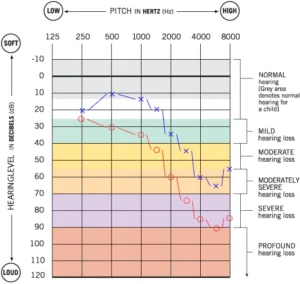
Audiograms Examples
Below are example audiograms for acoustic neuromas (AN) Remember these are examples and there will be variations in audiometric presentation for example where there is already an age-related hearing loss present, this is why you should always look at the onwards referral guidelines for post audiometry to see if the client meets the criteria for either asymmetry or deterioration.
| Example 1: Could be an example of an early found AN | Example 2 :Could be on an AN found with a worse hearing loss or watch and wait, where there may have been some progression in hearing loss |
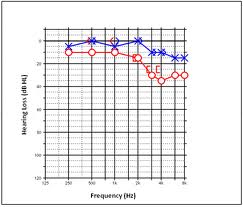
| Example 3: AN on right ear with age related loss |
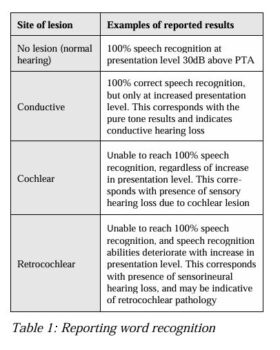
Speech Testing
Please note that speech testing can also indicate the possibility of an AN present. ‘Roll over’ is often found in clients with AN’s. ‘Roll over’ is when speech sounds are presented at levels where the client should hear well and respond with a good score but instead as the words are presented at louder levels the percentage correct lessens
‘Roll-over’ and is calculated by the following equation:
- Roll-over index = (maximum score minus minimum score) divided by maximum score
If roll-over is detected at a certain value (the value is dependent on the word list chosen for testing but is commonly larger than 0.4/0.45 AB word list as an example), then it is considered to be a sign of retro-cochlear pathology. If you look at the graph below the Y axis shows percentage correct and the X access the loudness as you can see for an AN as the sound is made louder there is a drop off in percentage correct rather than a plateau as there is for normal ears, conductive and cochlear loss hearing losses. Speech Audiometry PDF University of Cape Town

Intervention Options
Acoustic neuromas are generally managed in one of the following 3 ways. Which is chosen is dependent on the size and placement of the tumour, the clients/patient’s choices and recommendations by the ENT surgeon:
Watch and wait observation/monitoring with or without hearing aids (this will include ongoing MRI’s to check growth and notification of any changes in symptoms or growth shown on MRI to ENT) This is done more frequently in the below populations
- Elderly patients
- Patients with small tumours, especially if their hearing is good
- Patients with medical conditions that significantly increase the risk from an operation
- Patients who refuse treatment
- Patients with a tumour on the side of an only hearing ear
Stereotactic radiotherapy uses radiation delivered to a precise point or series of points in order to maximize the amount of radiation delivered to the acoustic neuroma tissue while minimizing the exposure of normal tissues nearby. It is commonly delivered as a single dose or less commonly, as multiple smaller doses. The goal is to stop tumour growth. People will need to be monitored with MRI scans after treatment to assess for any changes in size. In the UK we call this gamma knife and people often have to travel (referred to other centres) for this option.
Surgical removal is another treatment of for AN removal. The surgery can be conducted in different ways to remove the AN. How they approach the surgical removal of the AN depends on the location, size, hearing and facial nerve status as to which way is the best to access it. It is not unusual for surgery to involve Neurosurgeons along with the Ear, Nose and Throat Surgeons