Collapsed Ear Canals: Earmould impressions and hearing aid issues
Collapsed ear canals can be problematical when it comes to getting a well-fitting ear mould. The canal can neither be too long or too short. If either, then the earmould will be pushed out of the canal with jaw movement. A study in Brazil from 2017 suggested it occurs in on an average in 11% of clients. Statistically, they found it was between 3% – 36% across age groups with the largest percentage in individuals 75+ . Males are more likely to suffer from canal collapse. Ear canal collapse prevalence & associated factors among users of a centre of prevention and rehabilitation for disabilities
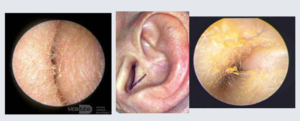
So how do you know if the ear canal is collapsing ? As shown in the 2nd image above.
Firstly, when doing otoscopy, we always look behind the ear for scars. Then we look straight into the canal. Often without first truly observing the canal and concha. I always tell my students to put some light pressure on the pinna to look to see if the ear canal is still remaining open. A collapsing canal will close further with just a little pressure, it will become a very narrow slit. You then know you have a collapsed canal.
Clients with collapsed canals may be more prone to wax accumulation (as it can’t exit the ear easily) but more importantly they may have issues with keeping hearing aids in their ears.
Open Fits/ Receiver-In-The Ear fittings with collapsing canals?
The client may be new to hearing aids and they wish to try an Open Fit or Receiver-In-The Ear with a dome; if their hearing loss allows. Or they already have hearing aids and prefer this option to an earmould. All you can both do is try and see if this works.
Be aware that you will need to have a trailing arm/tail on the wire to ensure that the wire and dome don’t push themselves out when the client speaks. See below image of what this tail looks like. I always say to these clients that this type of fitting may not work and you may need an earmould if we find it keeps pushing itself out. (This saves them having unrealistic expectations and getting upset when things don’t work)

So, they need an earmould … What advice would I give you?
When it comes to everyday impressions most earmould manufacturers preferred a closed jaw impression (the client doesn’t talk or move their jaw whilst the impression is setting).
This is fine when the client has a normal shaped canal or their canals are not highly mobile. However, as Ahead Simulations chart Earmold Impressions – AHead Simulations shows below you should always consider doing open jaw impressions if you have any of the below issues.
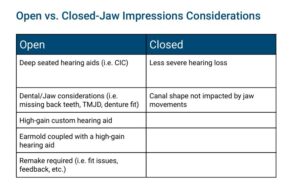
It is strongly advisable to take on open jaw impression for ears with collapsed canals, or highly mobile canals. In fact, I would suggest where you are up to your 3rd remake, comfort has been an issue or you know the canal is very mobile, then make both open and closed jaw impressions. Then the manufacturer can compare the two.
Also THINK! I made the mistake once of making sleep plugs for a client and not realising that she wore a mouth guard when sleeping. The sleep plugs didn’t work at all! I then made an open jaw impression which was consistent more with the shape of her canal when the mouth guard was in and hey presto it was a good fit! (she brought her mouth guard in to the 2nd appointment)
If the client wants a canal mould for a collapse canal, then the mould requires an anchoring point like a claw/spur as shown below.

How do I take an open jaw impression?
In order to take an open-jaw impression, a client opens their mouth wide using a bite bar before the impression material is injected. Keeps the bite bar in their mouth and this is not taken out till the impression material is fully cured.


A mouth prop can be bought from Impression Bite (25 Pack) – Puretone Shop
The recommended method according to the British Society of Audiology (BSA) is to insert the prop lengthwise in the corner of the mouth at the side the impression is taken as shown above. ‘For this process a dental mouth prop or bite-block should be placed between the subject’s side or rear teeth, after the otostop is inserted. (Reproduced with permission of Starkey Laboratories) A new and clean mouth prop should be used for each subject. The position of the otostop should be checked carefully using an otoscope when the mouth prop is in place to ensure there are no gaps between the otostop and the canal walls. The subject should be given a tissue to deal with any dribbling when the mouth prop is in place. Once the impression is set the mouth prop should be removed first. As the impression is likely to be a tight fit, extra care is required to ensure it is removed safely. With an open jaw it is particularly helpful if the subject moves their jaw gently from side to side during its removal’. (BSA Recommended Procedure 2023 Aural Impression Taking)
What next?
It may be a good idea to also make a closed jaw impression as well so the mould manufacturer can compare the two. Some people also do talking/moving jaw impressions, the thought is that the shape of the canal will be somewhere in between the two and give a more truthful impression of the ear canal.
At the moment it isn’t enough evidence to indicate whether there is a benefit to talking impressions over open jaw, so we are best to stay with the BSA recommendation of doing open jaw.
Basically, the rule of thumb is if they have had issues getting good moulds in the past, have collapsed canals or flatten conchae, or they have overly mobile canals (can check when doing otoscopy or they may have jaw issues that they have told you about) then do an open jaw impression.
Let the mould manufacturer know that is an open jaw impression, write as much information on the impression sticker to let them know of the issues (they don’t have a crystal ball) and then send on, and hopefully you should get a good earmould back that your client is happy with.
Lastly……
At some point soon will be a blog from me on canal collapse and the audiogram. I honestly believe this is an issue that is far too often missed by audiologists and audiometricians, resulting in clients being unnecessarily referred (and embarrassingly so) onto Ear, Nose and Throat Surgeons. Be prepared….. as I will definitely be on the soap box screaming on this subject!