In this article we will be looking at sudden sensorineural hearing loss. This is where the hearing has deteriorated/dropped suddenly within 72 hrs in one or both ears, and is not due to other issues such as wax, otitis media, infection etc. It is more often one ear, but it can be both. Please note that the BAA and NICE define it also define it as a rapid drop in hearing within the last 30 days or over a period of 3 days or less. Onward-Referral-Guidance-for-Adult-Audiology-Service-Users-Sept-23.pdf
This is an immediate urgent referral to Ear, Nose and Throat Teams. This can be done by a written/emailed letter from the GP. Or the client can go directly to A+E, or be seen privately by ENT. Private audiology services can directly refer to a private ENT ( I did this recently).
All NHS ENT clinics have emergency ENT appointments where clients can be seen same or next day for exactly this reason, pending a GP referral. The best outcome for clients is to be seen within 72 hrs and no later than 3 weeks. The outcome for clients seen after this time is not as good. Doctors urged to treat people with sudden hearing loss within seven days – RNID.
Grieving
I haven’t stated this in the previous blogs but it is worth remembering that counselling maybe required for clients with Acoustic Neuromas, Meniere’s Disease and Sudden Sensorineural Hearing Losses. We can often operate on otosclerosis and improve the hearing. But in the case of the above pathologies, we are potentially telling the client that they now have some form of permanent hearing loss.
They have gone from being ‘normal’ to no longer normal. People will often grieve this change, so it is important as their audiologist to understand this, support them as best you can, explain as much as you can and understand where they are on the grieving pathway. Some will move along this grieving pathway and come to some form of acceptance and some will get stuck in certain areas. This is normal reaction when a life change occurs, as their audiologist you cannot avoid these discussions, even if uncomfortable. Otherwise moving forward and helping support them to make appropriate choices in regards to their hearing care can’t happen effectively.
What is a sudden sensorineural hearing loss?
It is the rapid loss of hearing in one or both ears. It is typically one ear, but can be both. Bilateral involvement one article suggests occurs in 1–2% of patients. Acıpayam H, Koçak HE and Elbistanlı MS (2018) Sudden Sensorineural Hearing Loss. An Excursus into Hearing Loss. Available at: http://dx.doi.org/10.5772/intechopen.72219. Or possibly up to 5% according to one ENT.
Most commonly, a person will wake up and notice they can’t hear. In one case an ENT surgeon I knew, was driving on his way to his ENT clinic at the hospital and suddenly his hearing went in his right ear. I conducted a hearing test as soon as he arrived at work and it showed an almost complete hearing loss in the right ear.
British Academy of Audiology, NICE and ENT UK define sudden onset hearing loss:
- As a significant deterioration in hearing over 72 hrs or less, causing a noticeable hearing loss for most sounds
- The hearing loss may vary in severity.
- Many articles define it as a 30dB change in hearing at 3 consecutive frequencies
- A blocked or full feeling in the ear (aural fullness).
- Distortion of sounds in the poorer hearing ear.
- Tinnitus, which is the awareness of internal sounds in the ears or head.
- Nausea/vomiting.
Hearing loss, blocked feeling/aural fullness and tinnitus occur in 80% of SSHL. One study suggests that new/aural fullness that suddenly happens is one of the distinct signs of SSNHL and that quickness of presentation of aural fullness and hearing loss is not seen in other conductive pathologies. Dizziness or nausea tends to occur in about 30% of cases.
Presently the statistics point to 5-20 cases per 100,000 people each year. It is more often seen often in people between the ages 30-60, but can happen at any age and there is no difference in male /female susceptibility. However, we do know the incidence is rate is higher in the over 65’s.
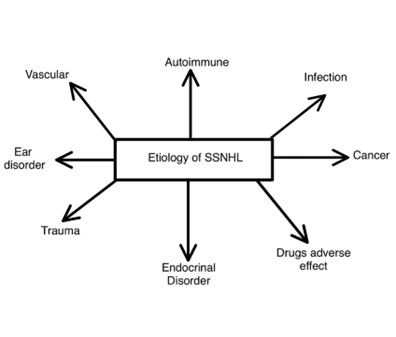
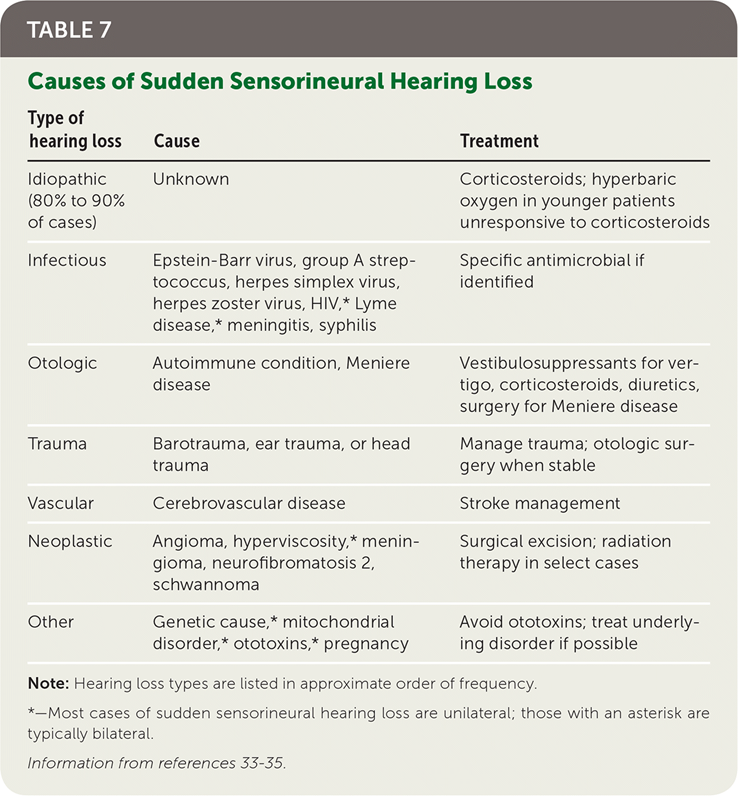
Sudden idiopathic hearing loss can happen if clients have multiple sclerosis, undiagnosed Cogan’s Syndrome Cogan’s Syndrome – Vasculitis UK. Most acoustic neuromas cause a gradual loss, a sudden hearing loss due to acoustic neuroma can also occur. Possible triggers for sudden sensorineural hearing loss are shown below. It is suggested that we are only able to find the cause of the sudden hearing loss in 10-15% of cases. This is why we call it a sudden idiopathic (unknown reason) hearing loss. Please note we can also add Covid 19 to the below chart.
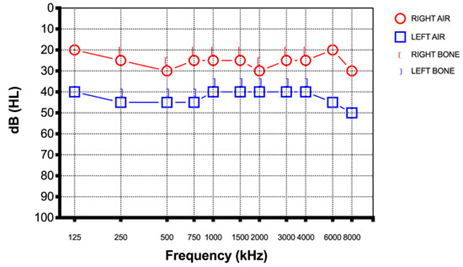
HEARING LOSS EXAMPLES
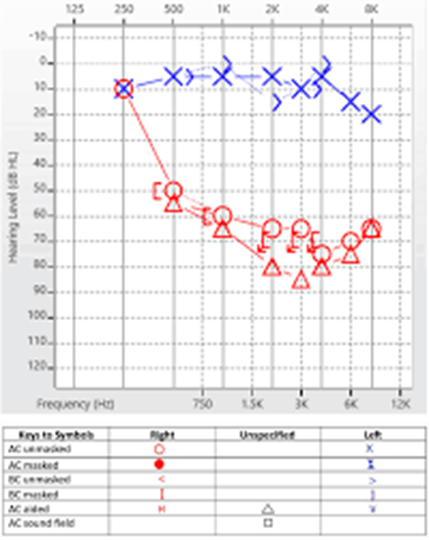
2nd Example

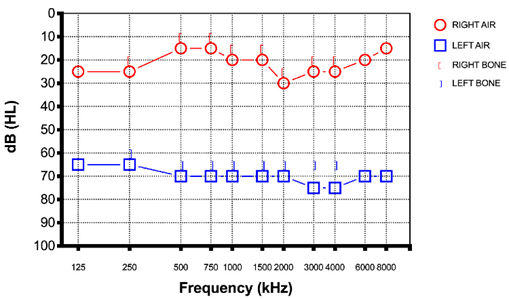
3rd Example
Checklist for clients who feel they have a sudden sensorineural hearing loss

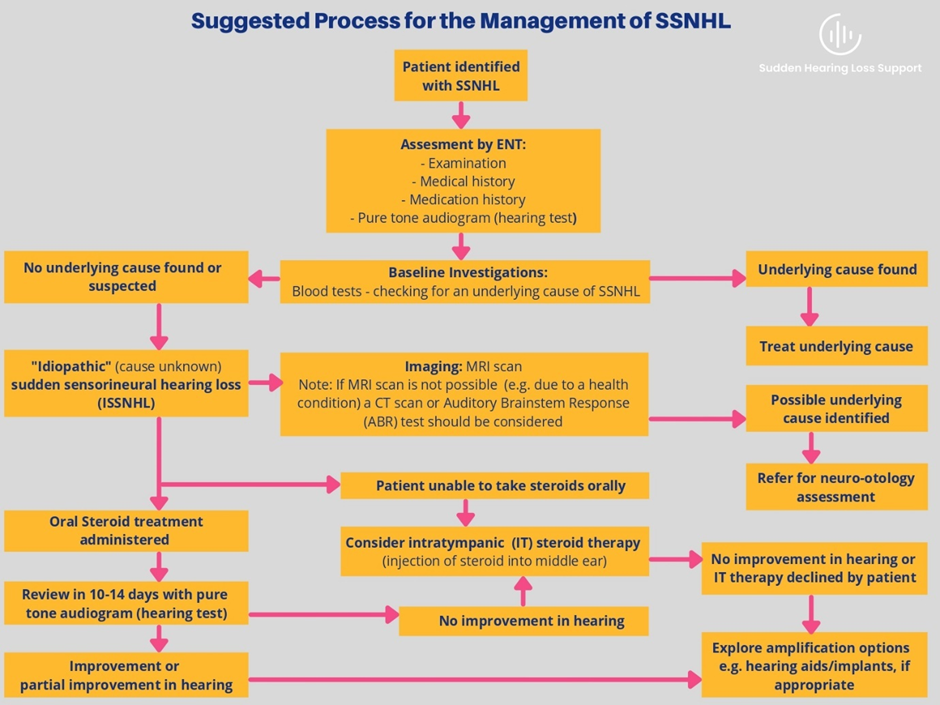
TREATMENT
Guidance in the British Journal of General Practice is as follows:
‘The time-critical treatment for SSNHL is the administration of steroids. This may be effective orally or when injected through the eardrum (intra-tympanic). In the primary care setting a short course of oral steroids (for example, prednisolone 1 mg/kg to a maximum 60 mg for 7 days) is recommended. Early treatment within 48 hours of onset of symptoms is ideal, while beyond 2 weeks it is considered no longer effective.’
STARFISH – INTEGRATE the STARFISH Trial: ‘Steroid Administration Routes for Idiopathic Sudden Sensorineural Hearing Loss’.
STARFISH is a randomised controlled trial designed to explore the effect of different steroid treatments for sudden sensorineural hearing loss. It is a UK-wide study funded by the National Institute for Health Research (NIHR). There is information for patients and medical and audiological individuals alike.

HEARING LOSS RECOVERY
Recovery of hearing in clients with SSNHL is not guaranteed, as it depends on the cause. Partial recovery of hearing can occur and more rarely total recovery. Presently there isn’t a definition amongst studies as to what recovery is. One study may use 30dB as an improvement, another 10dB. There are so many factors here such as age, underlying hearing loss; health issues all will have impact. 20240724-319105-v47d3j.pdf Sudden Sensorineural Hearing Loss in Patients Aged from 15 to 40 Years. The level of hearing loss, the frequencies that are affected, whether there is vertigo and the amount of time between when the sudden hearing loss happens and seeking therapy, will influence how the hearing recovers following a SSNHL.
According to the American Academy of Otolaryngology; patients with profound hearing loss, due to SSHL or patients who experience severe dizziness (vertigo) with their sudden hearing loss than those with no vertigo have a much lower chance of getting their hearing back. Along with individuals above age 65 and under 15. Patients with mid frequency hearing loss, particularly when hearing at 4000kHz was worse than 8000kHz, usually have a better prognosis
Lastly bilateral SSNHL tends to be more serious and is often related to systemic disorders (i.e. Multiple Sclerosis, Cogans) and generally has a worse prognosis. Please note in 20-30% of cases there is no improvement in hearing, regardless of whether intervention has occurred or not within the appropriate time period.
Improvement in hearing if it occurs, is often seen in the first 2-6 weeks after therapeutic intervention, but can take longer. If there is no change in the initial first 2 weeks, then research tends to suggest it is unlikely to improve significantly. Only around 36% have total recovery of hearing.
HEARING AIDS – A Cautionary tale (Speech Testing a must)
Presently all the research on sudden idiopathic hearing loss is geared towards understanding the causes and medical intervention, rather than the after effects.
Hearing aids are often recommended by ENT for clients after a sudden sensorineural hearing to help with the hearing loss left after medical intervention. As I indicated earlier a SSHL is a shock for the client and there is almost always some level of hearing loss post medical intervention (but perhaps less than there would have been with no intervention). The client will be grieving and therefore may pin all their hopes on a hearing aid restoring their hearing.
Three cautions here.
- A hearing aid is an aid to hearing and doesn’t restore hearing and has limitations in excessive noise and at a distance.
- Secondly, do a speech discrimination test on the affected ear: Whilst there isn’t much recorded research on this. Many of us in the know, are aware that speech discrimination can often be appalling on the SSHL ear. Particularly when the losses are flatter and moderate level losses onwards. Therefore, the outcome with hearing aids may be fairly limited. It may be best to go straight to a CROS or BICROS aids if the speech discrimination results are low, or are well worse than would be expected for the hearing loss. (Good PhD topic for anyone out there, there is virtually nothing written on this, except comments on forums and discussions between audiologists!)
- Distortion/Dysacusis/Diplacusis: Whilst this may be sometimes be a component of number 2 it can be of itself. Dysacusis is characterized by distortions in auditory perception, sounds may be perceived as distorted, unpleasant. This can manifest as echoic sounds, warbling tones, or a general metallic sound quality. Diplacusis is altered pitch perception. One ear may hear one pitch, while the other hears a different pitch. For SSHL clients with a music background this can have significant impact on their quality of life. Hearing Aids for Music – Exploring the music listening behaviour of people with hearing impairments
Unfortunately, I have seen many instances of aiding, where the affected ear has limited speech discrimination and sound is highly distorted for the individual. Even worse where the client has expected that the hearing aid would give them some clear sound. So please do a speech assessment. So that you and the client are clear on what the outcome with hearing aids will be. They may not wish to hear the truth, but it is better to know the outcome at the beginning then leading them on an upsetting journey.